urrently, competition at all societal levels is intensifying, subjecting some college students to multifaceted pressures. Consequently, mental health issues among these students are surfacing, with some progressing into mental disorders and illnesses. This phenomenon should not be underestimated in terms of its impact on both the affected students and others, and it directly exacerbates the challenges faced in student management within colleges and universities [1-3]. Consequently, the integration of mental health education into college student management is imperative to safeguard the holistic development of students’ physical and mental wellbeing, thereby enhancing the efficiency and quality of student management practices [4-6]. The incorporation of mental health education into college student management constitutes a systematic and comprehensive endeavor that necessitates sustained efforts for successful implementation. In this context, college student managers must maintain a keen understanding of students’ psychological dynamics and fluctuations in real-time, while establishing a scientific and practical operational framework to facilitate the achievement of college students’ physical and mental health development.
Mental health education entails the employment of diverse methodologies and measures, adhering to the principles of human psychological activities. It harnesses both internal and external factors to uphold individuals’ psychological well-being, fosters their positive psychological attributes, and enhances their overall development. As a novel educational concept, mental health education represents a multifaceted and multilevel educational system with profound implications [7-9]. Structurally, mental health education comprises two core aspects: psychological quality enhancement and mental health preservation, each addressing distinct developmental needs of individual students [10-12]. Psychological quality enhancement aims to empower students for success, whereas mental health preservation focuses on facilitating their normative growth, societal adaptation, and healthy adulthood. For college students undergoing physical and mental maturation, untimely management of acute stressors can lead to anxiety proliferation, ultimately triggering panic. Consequently, alleviating collective psychological anxiety among college students and exploring the establishment of an efficacious and high-quality mental health education model has emerged as a paramount priority in university mental health education [13-14]. Traditional mental health education models in universities have prioritized classroom-based theoretical instruction, complemented by targeted strategies like psychological counseling and extracurricular activities. However, integrating the SAFER-R model into mental health education, to bolster students’ psychological resilience and autonomy in everyday academic pursuits, necessitates innovative approaches to optimize mental health education in universities.
Literature [16] posits that mental health services facilitate the provision of a free and appropriate public education to students, emphasizing the necessity for district staff to be equipped to identify, assess, and cater to students with disabilities who may have mental health needs, subsequently developing individualized education plans tailored to their requirements. Literature [17] endeavors to discern specific school climate factors that potentially influence the interplay between adolescent health and development, as well as student identity formation. This study scrutinizes the relationship between students’ perceptions of school climate and their self-reported well-being, resilience, and moral identity, further delving into the interconnectedness among these three outcome variables. Meanwhile, Literature [18] employs structural equation modeling to conceptualize the extent of the relationship between crisis management, distance education practices, corporate image, and student satisfaction in higher education contexts, elucidating both direct and indirect effects among these variables. The findings reveal that students favorably assessed the university administration’s crisis management during the epidemic, with a concomitant enhancement in their perception of the organization’s image and overall satisfaction.
Literature [19] critically evaluates the formulation of a fall break policy at a mid-sized comprehensive university, uncovering inconsistencies in the labeling, scheduling, and evaluation of these breaks. These inconsistencies are identified as developmental flaws that could have been alleviated had faculty and student perspectives been incorporated into the policy-making process. Literature [20] underscores the significance of personality in facilitating the integration of experiential learning into the self-concept of management students. This work offers novel, practical, and empirically grounded insights for management educators on strategies to foster authenticity and mental well-being among students through innovative, engaging, and cost-effective online solutions. Literature [21] presents the findings of a questionnaire survey exploring college students’ mental health experiences and their access to mental health resources. The results indicate that stress is the preeminent mental health concern, with students expressing the greatest interest in learning techniques for balancing academic, work, and personal life, followed by stress management strategies. These findings provide valuable insights into students’ perceptions of mental health, which may inform and enhance outreach initiatives. Literature [22] details the outreach, education, and counseling efforts undertaken by college counselors, student affairs professionals, wellness coordinators, and administrators across the United States, emphasizing the training of students to identify and refer peers experiencing mental distress. However, the study notes a dearth of psychometrically sound methods to assist college counselors and student affairs professionals in assessing the potential reactions of students confronted with sexual harassment.
This paper investigates the feasibility of integrating mental health education into student management, leveraging the SAFER-R model as a framework to unite mental health education and student management, thereby fostering optimization and innovation within the context of a collaborative parenting model. It introduces a collaborative education framework specific to student mental health education, incorporates the beneficial aspects of the SAFER-R model, enhances the establishment of a school-centric mental health education and management system, and refines the management approach of the school’s mental health leadership team. Additionally, it advocates the utilization of data mining technology as a technical foundation for implementing personalized management education tailored to students’ mental health profiles. Experimental research is designed to process students’ baseline data, dissect their mental health characteristics, and evaluate the efficacy of student management within the collaborative education paradigm.
Mental health education is integrated into the process of student management, thereby significantly enhancing the overall quality of students and ultimately facilitating their holistic development in both physical and mental health.
Given that students in colleges and universities hail from diverse regions across the country, their living environments and habits vary significantly. Consequently, upon initially entering the institution, many students encounter discomforts and face the urgent need to adjust their emotions and mindsets across various aspects. In such circumstances, a subset of students with weaker mental resilience is prone to developing mental health issues. Consequently, the focus of student management in colleges and universities ought to shift towards addressing and guiding the psychological well-being of new students. However, some institutions have overlooked this issue, and in some cases, have even omitted mental health education altogether.
The emotional issues of college students have consistently garnered significant attention due to their heightened sensitivity, particularly because they are traversing the tumultuous period of adolescence, where both physical and psychological development attain a relatively mature stage. Consequently, they often harbor interest and anticipation towards the opposite sex, necessitating proactive guidance and intervention to address mental health concerns stemming from emotional turmoil or the frustration that may accompany these experiences. Furthermore, a notable subset of college students becomes overly engrossed in their romantic lives, neglecting academic pursuits, ultimately fostering an unhealthy psychological landscape and, in extreme cases, predisposing them to aggressive behaviors when confronted with emotional difficulties.
Indeed, the Internet abounds with positive information; however, it also harbors a significant amount of unhealthy and detrimental content, alongside online games and other distractions. College students, being the primary audience of the Internet, often succumb to excessive indulgence, ultimately leading to the neglect of their academic pursuits. A portion of university student management endeavors are often implemented in a mandatory fashion, where some administrators fail to delve deeply into the psychological dynamics of students. They overlook the contemporary psychological landscape of college students and persist in adopting traditional perspectives and mindsets towards them. This approach directly contributes to the delayed integration of student management and mental health education within colleges and universities, yielding suboptimal outcomes that often fall short of expectations and, in some cases, elicit resistance from students.
In response to the aforementioned exploration regarding the integration of mental health education and student management, this paper proposes the adoption of the SAFER-R model as a means to unify these two domains, thereby innovating the collaborative educational model and achieving a synergistic approach to their education.
The concepts in the SAFER-R model have wide applicability for college student groups to cope with unexpected situations.
As specialists in psychological intervention, they must adhere to certain working principles, among which are the principles of immediacy, proximity, simplicity, and brevity. This set of principles, commonly referred to as the PIE principle, emphasizes fostering individual psychological flexibility and resilience.
Given the distinct group characteristics of college students, constrained by age and experiential limitations, they are susceptible to impulsivity when confronted with certain issues. Therefore, when implementing the SAFER-R model, the primary objective is to stabilize the service recipients, embodying the essence of the model’s initial letter ’S’ for Stabilize. This stabilization process fosters clear thinking and an enhanced sense of reality, thereby enabling the mobilization of energy and capabilities necessary for an effective response.
In the SAFER-R model, the ’A’ stands for Acknowledge, which involves recognizing the unexpected situation and harnessing knowledge reserves to rationally comprehend the prevailing phenomena, problems, individuals, and events, along with one’s own capabilities. During this process, the helper must comprehend two key aspects through the narrative provided by the individual: firstly, the process itself and secondly, the physical and psychological reactions experienced by the individual, specifically, the manner in which they responded during the event.
In the SAFER-R framework, the ’F’ represents Facilitate Understanding, which involves utilizing the information gathered during the preceding stages to deepen comprehension of the “abnormal reactions” exhibited across the five domains of cognition, emotion, physicality, behavior, and the three perspectives (outlook on life, values, and worldview). It is crucial to recognize that these reactions, though seemingly abnormal, are often “normal responses to abnormal events.”
E-Encourage effective coping in SAFER-R means to encourage effective coping, to help college students focus on what they can control, to help them find a sense of internal control, and to help them strengthen their “internal and external resources,” which requires a social work strengths perspective to help them see resources. It requires a social work strengths perspective to help them see resources. As a helper, it is important to have a pair of eyes that are good at finding resources.
The R-Recovery of Referral in SAFER-R means referral, knowing that under the same incident, everyone’s coping and endurance are different, and if we really assess that the students need to be referred to the higher level of psychotherapy or medication, so that we can help them in a better and more timely manner, we, as a helper, need to have the ability to make such an assessment.
The concepts in the SAFER-R model can be applied to the mental health education model of college students, which can not only enhance students’ psychological resilience, but also improve their ability to cope with emergencies, which can promote their healthy and comprehensive growth.
Mental health education can accompany the growth and success of college students, motivating them to enhance themselves and attain their personal aspirations, thereby laying a solid foundation for them to become pillars of society.
College students are inherently characterized by complexity, diversity, and individuality. Amidst the rapid proliferation of new media networks, they are exposed to an increasingly fragmented array of information, subtly transforming their values, consumption patterns, and aesthetic preferences. Consequently, numerous and intricate psychological issues have arisen, emphasizing the paramount importance of establishing a robust mental health education framework tailored specifically for college students.
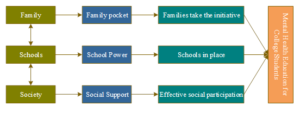
Mental health education for college students constitutes a comprehensive and systematic endeavor, necessitating the establishment of educational synergies, the construction of collaborative mechanisms, and the optimal utilization of multiple stakeholders to collectively advance the development of this vital area. Throughout the trajectory of college students’ growth and achievement, the family serves as a pivotal arena for personality cultivation, with familial factors often being a significant contributor to psychological challenges faced by students. Conversely, the school represents the primary locus of instruction and moral upbringing, occupying a central role in the ideological, political, and mental health education of college students. Meanwhile, society functions as the external milieu within which mental health education unfolds, with social environments and support networks constituting direct influences on students’ psychological well-being. Consequently, it is imperative to integrate the human resources of the family, school, and society to forge a cohesive, tripartite mechanism for mental health education among college students, grounded in the principles of “family support, school support, and social support.”
The implementation framework of the synergistic mechanism for mental health education among college students is depicted in Figure 1. This mechanism establishes a multi-faceted community of mental health education, fostering enhanced educational collaboration. It facilitates comprehensive, effective, and diversified mental health education for college students, thereby offering valuable guidance and support in this critical area.
Mental health education constitutes a systematic, extensive, and highly specialized endeavor that necessitates the concerted efforts and collaboration across all levels and facets of the institution. This necessitates the cohesive alignment of various forces, the mobilization of relevant departments and personnel, as well as the establishment of a robust and stable operational framework to ensure security and continuity. Given its profound implications for students’ physical and mental wellbeing, mental health education demands a dedicated leadership that accords it paramount importance, demonstrating both boldness and resilience. Ideally, it should be prioritized and integrated into a select few strategic initiatives to ensure its effectiveness and impact.
Schools should establish a comprehensive mental health education work system that outlines clear work content, workflows, and work standards. This system should provide guidelines for addressing students who exhibit signs of mental health issues, ensuring the development of standardized operating procedures and workflows for effective intervention.
During the initial month of freshman enrollment, the university conducts a comprehensive mental health assessment for all incoming freshmen. This assessment aims to gain insight into the mental wellbeing of the entire cohort, identify students requiring attention, establish individual health profiles, and subsequently implement follow-up measures as necessary.
For the graduating cohort, the institution will undertake a comprehensive assessment of all students, comparing the outcomes of the initial enrollment assessment with the current results. This evaluation aims to discern the progression of students’ mental health over time and, concurrently, to scrutinize and evaluate the efficacy of the school’s mental health education programs. The purpose is to identify areas of deficiency and implement timely enhancements to optimize the support provided.
Concurrently, the assessment of graduating students also emphasizes on assessing their mental health readiness for societal integration and employment, thereby enabling the timely identification of students facing challenges and the subsequent provision of tailored interventions and guidance.
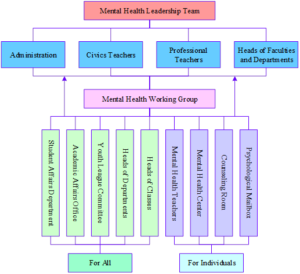
The School Mental Health Leadership Team management model is shown in Figure 2.
Responsibilities and tasks at all levels and departments:
The responsibilities of the leading group encompass the following key aspects: according paramount importance to the task, formulating pertinent rules and regulations, engaging in systematic planning, as well as organizing and executing the implementation process.
Responsibilities of the working group: implementing work responsibilities, professional team building, work performance assessment, and developing work plans.
The Mental Health Education Center aims to facilitate the development of mental health professional curricula, meticulously select appropriate teaching materials, devise comprehensive mental health work routines, and curate thematic educational activities. It oversees the guidance of mental health educators in conducting psychological counseling sessions and managing psychological assistance platforms, such as mailboxes. Furthermore, the Center endeavors to identify students facing potential issues, promptly intervene, and provide effective guidance and support.
Responsibilities of the Student Affairs Office encompass effectively facilitating the development of a cohesive classroom teacher team, closely monitoring and supporting students with mental health concerns, and collaborating with the Mental Health Education Center to implement comprehensive mental health education initiatives.
The Academic Affairs Office is tasked with organizing and facilitating mental health education within the classroom setting, while also collaborating with the Mental Health Education Center to provide guidance to specialized educators in effectively integrating mental health content into their curricula.
The Youth League Committee endeavors to enhance the diversity and effectiveness of club organizations, organizing a myriad of activities aimed at fostering students’ positive psychological attributes. Furthermore, it leverages student groups as a means to identify issues promptly and report them in a timely manner.
Class teachers implement mental health education seamlessly into the daily management and educational activities of their respective classes, thereby raising awareness of mental health among students. In their routine duties, these educators are adept at detecting potential psychological issues manifested in students’ daily behaviors. Upon identification, they promptly notify the Mental Health Education Center and collaborate closely with the center in providing psychological counseling and guidance to the affected students.
In the realm of data mining technology, the primary algorithms employed encompass the decision tree algorithm, association rule algorithm, neural network algorithm, genetic algorithm, Bayesian network algorithm, along with various statistical analysis methods. For the purpose of conducting data analysis research pertaining to students’ mental health, this paper selectively utilizes the decision tree C4.5 algorithm and the association rule Apriori algorithm.
)1) C4.5 algorithm is a decision tree algorithm improved on the basis of the original ID3 algorithm. The principle of ID3 algorithm is as follows: Suppose \(S\) is a collection of \(s\) data samples. Then have \(m\) different values for the class attribute: \(C_{i} \left(i=1,2,\ldots ,m\right)\). Let \(s_{i}\) be the number of samples in class \(C_{i}\). The total information entropy for this given sample is: \[\label{GrindEQ__1_} I\left(s_{1} ,s_{2} ,\ldots ,s_{m} \right)=-a_{i=1}^{m} P_{i} \log _{2} \left(P_{i} \right) , \tag{1}\] where \(P_{i}\) is the probability that any sample belongs to \(C_{i}\), which can usually be expressed as \(\frac{s_{i} }{s}\).
Suppose attribute \(A\) has \(k\) different values \(\left\{a_{1} ,a_{2} ,\ldots ,a_{k} \right\}\), set \(S\) is divided into \(k\) subsets \(\left\{S_{1} ,S_{2} ,\ldots ,S_{k} \right\}\) by attribute \(A\), and samples in set \(S\) where attribute \(A\) takes the value \(a\), are included in subset \(S\), among others. If it is determined that the test attribute is attribute \(A\), then the new leaf node generated from this set node is the above subset. Let \(s_{ij}\) be the number of samples of category \(C_{i}\) in subset \(S_{j}\), and the value of information entropy of the samples is obtained by division: \[\label{GrindEQ__2_} E\left(A\right)=a_{j=1}^{k} \frac{s_{1j} +s_{2j} +\ldots +s_{mj} }{s} I\left(s_{1j} ,s_{2j} ,\ldots ,s_{mj} \right) . \tag{2}\] Among them, \[\label{GrindEQ__3_} I\left(s_{1j} ,s_{2j} ,\ldots ,s_{mj} \right)=-a_{i=1}^{m} P_{ij} \log _{2} \left(P_{ij} \right) . \tag{3}\] \[\label{GrindEQ__4_} P_{ij} =\frac{s_{ij} }{s_{1j} +s_{2j} +\ldots +s_{mj} } . \tag{4}\] Eq. (4) is the probability of a sample of category \(C_{i}\) in subset \(S_{j}\). Finally, the information gain (Gain) of sample set \(S\) is obtained by dividing: \[\label{GrindEQ__5_} Gain(A)=I\left(s_{1} ,s_{2} ,\ldots ,s_{m} \right)-E(A) . \tag{5}\] It is shown that if the value of information entropy \(E\left(A\right)\) becomes smaller, the value of information gain \(Gain\left(A\right)\) becomes larger. As one of the more typical learning algorithms in decision trees, the ID3 algorithm focuses on using the information gain of the nodes to determine the measurement attributes, allowing for a maximum category classification gain to be obtained when computing all non-leaf nodes, which in turn allows the dataset to have a minimum entropy after classification. The general depth of the tree is reduced by this solution, allowing a reasonable increase in classification efficiency.
The C4.5 algorithm has mainly made the following adjustment changes:
a) Addresses the drawback of insufficient attributes in the ID3 algorithm by introducing information gain rate, which mainly focuses on identifying attributes with multiple values as split attributes through information gain.
b) Has the ability to process operations on continuous and discrete attribute types, i.e., discretization operations can be performed on continuous attributes.
c) Performs pruning operations after constructing a decision tree.
d) Training samples with missing attribute values can be processed.
The C4.5 algorithm is usually the information gain rate of the attributes instead of the information gain, and the highest value is determined as the test attribute by calculating the information gain rate of all the attributes. By this way, the branch nodes of the decision tree are generated, and the branches of the decision tree are accordingly generated by the attributes with different values, and each branch represents a subset of the samples divided.
The decision tree based C4.5 algorithm operates as follows:
Step 1: Firstly, the information gain rate of each split attribute in the training sample set is obtained by calculation.
Step 2: The root node of the decision tree is determined by the split attribute with the maximum information gain rate, and the data set is split into corresponding sub-data sets according to the number of values taken.
Step 3: Steps 1 and 2 are performed sequentially and recursively in the sub-dataset.
3) Association rules and frequent itemsets: The probability that both itemset A and itemset B occur together is called the support of the association rule, also known as relative support: \[\label{GrindEQ__6_} \text{Support}\left(A\Rightarrow B\right)=P\left(A\cap B\right), \tag{6}\] When itemset \(A\) occurs, the probability that itemset \(B\) also occurs is the confidence level of the association rule: \[\label{GrindEQ__7_} \text{Confidence}\left(A\Rightarrow B\right)=P\left(B\left|A\right. \right) . \tag{7}\]
The term “minimum support” is frequently utilized to denote the threshold employed in defining the measure of support, representing the minimal statistical significance standard required for an itemset within the dataset. Similarly, the “minimum confidence level” is commonly referred to as the threshold that establishes the minimum reliability criterion for association rules, signifying the level of confidence required for the rule. Rules that meet both the minimum support threshold and the minimum confidence threshold are typically classified as strong rules.
If the support counts of the itemsets are known, the support and confidence of Rule \(A\Rightarrow B\) can be deduced from the counts of all transactions, the support counts of itemset \(A\) and itemset \(A\cap B\): \[\begin{aligned} \label{GrindEQ__8_} {\text{Support}\left(A\Rightarrow B\right)} {=} {\frac{\text{Number of simultaneous transactions} A,B} {\text{Number of all transactions}} } {=} {\frac{\text{Support count}\left(A\cap B\right)}{\text{Total count}\left(A\right)} }. \end{aligned} \tag{8}\] \[\begin{aligned} \label{GrindEQ__9_} {\text{Confidence}\left(A\Rightarrow B\right)} {=} {P\left(B\left|A\right. \right)} {=} {\frac{\text{Support}\left(A\cap B\right)}{\text{Support}\left(A\right)} } {=} {\frac{\text{Support count}\left(A\cap B\right)}{\text{Support count}\left(A\right)} }. \end{aligned} \tag{9}\]
By obtaining the support counts for all transactions, \(A\), \(B\) and \(A\cap B\), the corresponding association rules \(A\Rightarrow B\) and \(B\Rightarrow A\) can be generated, which ultimately determines whether or not they are strong association rules.
Collaborative education models in mental health prioritize a “people-centered” approach, and the evolution from mental health education towards mental health management services represents an inevitable trend in this field. From a big data perspective, the realization of personalized mental health services and the facilitation of precise and refined educational management constitute crucial aspects of mental health work. This approach can effectively mitigate the risk of accidents arising from psychological issues experienced by contemporary postgraduates, who often face significant pressures in their personal and academic lives.
Firstly, leveraging the vast information garnered through big data technology, it is imperative to promptly conduct research, analysis, and evaluations to comprehend the individual needs of students and subsequently offer them tailored mental health services that are uniquely suited to each student’s requirements.
Secondly, when utilizing the Internet, artificial intelligence, big data, and other emerging technologies to predict psychological issues among college students, it is essential to attain precise identification and implement targeted solutions. Solutions should be devised in accordance with the categorization and severity levels of individual students’ mental health conditions. Furthermore, it is imperative to promptly address any difficulties or psychological crises encountered by students, striving to mitigate the potential impact of such crises to the greatest extent possible.
In fields such as sociology, psychology, and economics it is often necessary to study the probability of an event occurring and to discuss what factors are associated with the magnitude of that probability. However, if the study is done directly using the value of \(p\) as the dependent variable, there are two difficulties in dealing with it. First, the range of values of \(p\) makes it impossible to express its relationship with the independent variable in a linear model. The second is that \(p\) varies so little around 0 or 1 that ordinary methods cannot cope with this variation. Therefore, a transformation is needed such that it is a monotonic function (denoted \(Q\left(p\right)\)) of values of \(p\), which should take as large a range of values as possible, and which is sensitive to recognizing when \(p\) varies slightly near 0 or 1, i.e., \(\frac{dQ}{dp}\) is proportional to \(\frac{1}{p\left(p-1\right)}\).
It may be desirable to make: \[\label{GrindEQ__10_} Q=\ln \frac{p}{\left(1-p\right)}. \tag{10}\]
When \(p\) is from \(0\to 1\), \(Q\) is from \(-\infty \to +\infty\), i.e., the interval of values of \(Q\) is \(\left(-\infty ,+\infty \right)\). This transformation completely solves the two difficulties mentioned above and is much more convenient to deal with, and it is called the \(Logit\)-transformation, viz: \[\label{GrindEQ__11_} Logit\left(p\right)=\ln \frac{p}{1-p} . \tag{11}\]
In the specific modeling process, it is first fitted: \[\label{GrindEQ__12_} Q=\ln \frac{p}{\left(1-p\right)} . \tag{12}\]
The equation between Eq. (12) and the independent variable, and then according to the functional relationship between \(Q\) and \(p\), the relationship between \(p\) and the independent variable is introduced.
In real life, there are usually more than one influencing factors, denoted as \(x_{1} ,x_{2} ,\ldots ,x_{k}\). These independent variables can be qualitative or quantitative data, if the following conditions are satisfied between the independent variables and the dependent variable: \[\label{GrindEQ__13_} \ln \frac{p}{\left(1-p\right)} =b_{0} +b_{1} x_{1} +b_{2} x_{2} +\ldots .+b_{k} x_{k} . \tag{13}\]
That is, \(\ln \frac{p}{1-p}\) is a linear function of \(x_{1} ,x_{2} ,\ldots ,x_{k}\), then it is called Logistic linear regression.
If there are \(n\) samples with \(k\) observations each, the corresponding Logistic regression model has the following form: \[\label{GrindEQ__14_} \ln \left(\frac{p_{i} }{1-p_{i} } \right)=b_{0} +\sum _{i=1}^{k}b_{k} x_{ik} . \tag{14}\]
Among them, \[\label{GrindEQ__15_} p_{i} =P\left(y_{i} =1\left|x_{i1} ,x_{i2} ,\ldots ,x_{ik} \right. \right) . \tag{15}\]
Eq. (15) is the probability of occurrence of the object of study given the value of the independent variable \(x_{i1} ,x_{i2} ,\ldots .,x_{ik}\).
In this chapter, we will delve into the application of data mining in mental health management, adhering to the standard data mining process. Specifically, we will employ the matrix-based Apriori algorithm to identify frequent itemsets, thereby uncovering the underlying association rules between psychological factors. Furthermore, we will utilize the decision tree algorithm to construct decision trees and generate classification rules. These derived rules will enable us to analyze potential relationships between psychological factors and students’ basic information. Concurrently, the obtained decision tree model will be leveraged to classify and predict new data, ultimately providing a scientific and objective basis for decision-making in student psychological counseling.
In this paper, our mining object comprises the psychological data generated from the psychological census conducted among the 2022 student cohort of a specific college during their enrollment. This cohort encompasses a total of 2807 students, with a breakdown of 1062 males and 1745 females, distributed across eight faculties: the Department of Tourism Management, the Department of Hospitality Management, the Department of Tourism and Foreign Languages, the Department of Economics and Trade, the Department of Social Services, the Department of Food Science and Technology, the Department of Information Engineering, and the Department of Mechanical and Electrical Engineering.
In this study, the admission assessment data from the Symptom Self-Rating Scale SCL-90, administered during the psychological census test for the class of 2022 students at the time of freshman admission, were selected as the research dataset. The Apriori algorithm was employed to mine the interconnections among the psychological factors within the SCL-90. Additionally, the Decision Tree algorithm for classification analysis was utilized to explore potential relationships between the SCL-90 scores and students’ basic information. Subsequently, the obtained results were analyzed and interpreted.
SQL Server 2022 is employed for data storage, utilizing a relational data model. The student’s personal basic information, which is synchronized from the academic staff system, captures the fundamental details of each student. This information encompasses student number, name, gender, date of birth, ethnicity (coded for simplicity), place of origin, faculty, major, status as an only child, family economic income, and whether the student comes from a single-parent household. Several items within the basic personal information have been streamlined through the use of codes, including ethnicity and specialty.Additionally, a table detailing students’ personal psychological issues is generated by the psychological assessment system. This table captures the students’ propensity towards experiencing psychological problems, as reflected by their current scores across nine psychological dimensions: hostility, anxiety, psychoticism, terror, paranoia, obsessive-compulsive symptoms, somatization, interpersonal sensitivity, and depression. The school number serves as a common identifier linking this table with the personal basic information.
The structure of the data table pertaining to students’ personal basic information is presented in Table 1. This table maps the students’ personal basic data onto respective field names, facilitating their seamless utilization in data processing tasks. Specifically, within the table, “JJ” serves as an abbreviation for “family economic income,” and the maximum length allocated for this field is 30 characters.
| Field name | Meaning | Data type | Maximum length |
| XH | School number | Fixed string | 10 |
| XM | Name | Fixed string | 12 |
| XB | Gender | Fixed string | 3 |
| SR | Date of birth | Date | 5 |
| MZ | Peoples | Fixed string | 9 |
| SYD | Biotically | Fixed string | 10 |
| YX | Hospital system | Fixed string | 25 |
| ZY | Majors | Fixed string | 25 |
| DS | The only child | Fixed string | 28 |
| JJ | Household income | Fixed string | 30 |
| DQ | Single parent | Fixed string | 25 |
The structure of the data table outlining students’ personal psychological problems is presented in Table 2. This table categorizes the students’ personal psychological issues into nine distinct domains: hostility, anxiety, psychoticism, phobia, paranoia, obsessive-compulsive symptoms, somatization, interpersonal sensitivity, and depression.
| Field name | Meaning | Data type | Maximum length |
| XH | School number | Fixed string | 10 |
| DD | Antagonism | Numerical type | 5 |
| JL | Anxiety | Numerical type | 5 |
| JSBX | Insanity | Numerical type | 5 |
| KB | Horror | Numerical type | 5 |
| PZ | Paranoia | Numerical type | 5 |
| QPZZ | Obsessive-compulsive disorder | Numerical type | 5 |
| QTH | Somatization | Numerical type | 5 |
| RJGX | Interpersonal sensitivity | Numerical type | 5 |
| YY | depression | Numerical type | 5 |
During the initial screening of the data, a substantial amount of problematic and irrelevant data is encountered, which not only prolongs the data mining process but also introduces potential biases into the mining results. By conducting a pre-screening of the initial data, eliminating invalid entries, and thereby reducing the duration of the screening process, the overall quality of the database can be significantly enhanced.
Data selection: The effective way to shorten the data mining time is to pre-process the whole database object, and the processing has the initial screening to remove those useless data. In order to extract high quality data, the data is processed as follows:
The personal information form filled out by the students was processed to remove the student’s name, student’s age, field of study, contact information, and other factors in the form that are not related to this data screening.
The ethnicity of the students in the form was excluded because Han Chinese accounted for more than 90% of all students, so this option was invalid data and was excluded.
The options related to the psychological characteristics of the study were screened for their relevance.
Finally, the factors related to mental health of the study are determined, and the data set of the study of psychological conditions is composed.
Application of Apriori algorithm in psychological assessment: Given the unique characteristics of students’ psychological assessment, the Apriori algorithm has been selected as the primary tool for realizing this assessment. Traditionally, the Apriori algorithm relied on a recursive mechanism, which necessitated scanning the entire database each time a frequent itemset was computed, resulting in significant time consumption. To address this issue, an improved Apriori computation method under matrix conditions has been employed. This approach facilitates the screening of students’ psychological data and the identification of associations among various psychological dimensions.Focusing on the matrix-based computation of the Apriori algorithm, the process involves organizing the data into a matrix format. Subsequently, the support counts for each itemset are derived through the inner product operation of vectors, leveraging the computational power of matrix methods. This ultimately leads to the formation of a set of options that are then divided into the following three distinct steps:
a) Transform the thing data to form a Boolean matrix.
b) Automatically concatenate frequent itemset \(L_{K}\) to compute candidate itemset \(C_{K+1}\).
c) Count all the itemsets in the candidate itemset to generate the frequent itemset.
By utilizing the matrix-based Apriori algorithm for data mining, some of the association rules between the nine psychological symptom factors are shown below:
\(jl2,dd2\Rightarrow qpzz2\) Confidence (conf) 0.91 Support (sup) 0.22.
\(yy2,jl2\Rightarrow qpzz2\) Confidence (conf) 0.95 Support (sup) 0.27.
\(jl2,jsbx2\Rightarrow yy2\) Confidence (conf) 0.85 Support (sup) 0.25.\(qpzz1,pz1\Rightarrow qth1\) Confidence (conf) 0.97 Support (sup) 0.47.
\(qpzz1,rjgx1\Rightarrow qth1\) Confidence (conf) 0.98 Support (sup) 0.41.
\(qpzz1,pz1\Rightarrow rjgx1\) Confidence (conf) 0.90 Support (sup) 0.38.
\(yy2,dd2\Rightarrow jl2\) Confidence (conf) 0.89 Support (sup) 0.26.
The rules are converted into values in the form of code lists, which are then stored in a rule base with associations. The objects in the rule base are then analyzed to find out their internal associations to obtain the rule, and the final result is that students suffering from obsessive-compulsive disorder (OCD) are very likely to have symptoms of depression, anxiety, interpersonal sensitivity, and paranoia as well. The students with symptoms of interpersonal sensitivity also had a higher probability of having symptoms of somatization and paranoia. By analyzing this data, it was concluded that there is some hidden correlation between psychological latitudes, and that detecting these correlations in advance can help prevent the emergence of mental illness.
Regarding the psychological status of college students, the dataset analyzed in this study comprises 7013 samples pertaining to college students’ mental health. Among these samples, 4320 (61.60% of the total) exhibit no psychological problems, whereas 2693 samples (38.40% of the total) reveal the presence of psychological issues.
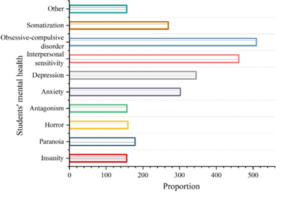
As evident from the SCL-90 Symptom Self-Assessment Scale’s rating scale, a mean score exceeding 2 in a factor indicates heightened distress and a greater likelihood of psychological problems in that area among students. Consequently, the mental health dataset analyzed in this study categorizes and tallies the different influencing factors, specifically identifying those with mean scores above 2. The resulting visualization of students’ mental health data is presented in Figure 3. Notably, the mental health status of students in this school is characterized by a prominence of obsessive-compulsive symptoms, followed by interpersonal sensitivity, depression, and anxiety, with specific distributions of 509 for obsessive-compulsive symptoms, 461 for interpersonal sensitivity, 345 for depression, and 302 for anxiety. While psychoticism, hostility, and terror exhibit a lesser influence compared to the aforementioned factors, their significance should not be overlooked as they still constitute an essential aspect of students’ mental wellbeing.
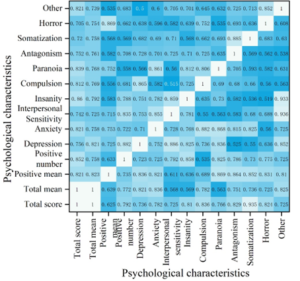
In this study, a comprehensive analysis was conducted on 14 variables that impact the mental health of college students. These variables encompass total score, total mean score, mean score of positive items, number of positive items, as well as specific factors such as depression, anxiety, interpersonal sensitivity, psychoticism, obsessive-compulsive disorder, paranoia, hostility, somatization, horror, and others. To investigate the extent of correlation among these variables, a heat map was generated utilizing Pearson correlation coefficients. The heat map visually represents the correlations among the students’ psychological characteristics, with the intensity of correlation indicated by the heat values, as presented in Figure 4.
As evident from Figure [X], all variables exhibit a correlation coefficient exceeding 0.5, indicating a relatively strong correlation among them. Notably, the correlation coefficients for total score, total mean score, depression, anxiety, number of positive items, interpersonal sensitivity, and psychoticism surpass 0.7, signifying an even stronger association. In particular, the correlation coefficient between interpersonal sensitivity and depression is 0.886, indicating a highly significant correlation. In contrast, while the remaining variables also display a positive correlation, their coefficients are not as pronounced as those mentioned above.
| Dependent variable | Predictor variable | $$R^2 $$ | $$F$$ | $$Beta$$ | $$t$$ | $$P$$ |
| Values | Male vs Female | 0.023 | 5.351 | -0.125 | -3.826 | 0.043 |
| Science and engineering students vs arts and crafts students | 0.061 | 5.618 | 0.186 | 3.245 | 0.009 | |
| Arts students vs arts and crafts students | 0.152 | 3.621 | 0.004 | |||
| Cognition | Sophomore vs Freshman year | 0.032 | 12.054 | 0.153 | 3.265 | 0.001 |
| Junior vs Freshman year | 0.352 | 4.596 | 0.005 | |||
| Senior year vs Freshman year | 0.396 | 4.002 | 0.003 | |||
| Action performance | Science and engineering students vs arts and crafts students | 0.059 | 12.338 | 0.168 | 2.965 | 0.001 |
| Arts students vs arts and crafts students | 0.304 | 3.507 | 0.001 | |||
|
Inventory
of total |
Science and engineering students vs arts and crafts students | 0.73 | 12.372 | 0.163 | 3.205 | 0.045 |
| Arts students vs arts and crafts students | 0.367 | 5.138 | 0.000 |
| Project | Serial number | Survey content | Evaluation (%) | |||
| Good | Better | General | Difference | |||
| Evaluation of mental health education Settings | 1 | Mental problem solving | 35.6 | 39.3 | 22.5 | 2.6 |
| 2 | The course arrangement is reasonable | 22.5 | 64.7 | 9.5 | 3.3 | |
| 3 | Compliance with your own professional learning | 34.7 | 55.1 | 6.8 | 3.4 | |
| 4 | Satisfaction with the form of mental health education | 40.2 | 41.7 | 12.3 | 5.8 | |
| Personal ability to improve in school | 5 | Professional practice | 76.1 | 8.7 | 10.5 | 4.7 |
| 6 | Social ability | 56.9 | 32.1 | 5.8 | 5.2 | |
| 7 | Organizational management | 52.3 | 25.2 | 15.8 | 6.7 | |
| 8 | Interpersonal skills | 54.0 | 27.2 | 15.2 | 3.6 | |
| 9 | Mental quality | 50.1 | 33.8 | 12.4 | 3.7 | |
| 10 | Performance ability | 57.5 | 27.3 | 12.6 | 2.6 | |
In the multiple regression analysis, if the independent variables (gender, grade and major) are intermittent variables, they should be converted into dummy variables in the input regression model in order to make the intermittent variables have the characteristics of continuous variables, and then the converted dummy variables should be used as one of the predictor variables in the multiple regression. The results of the regression analysis after gender, grade and major have been transformed are shown in Table 3, indicating that male students have more negative values and female students have healthier values compared to female students. \(R^{2}\)=0.023, \(F\)=5.351, \(Beta\)=-0.125, \(t\)=-3.826, \(P\)=0.043. sophomores, juniors, and seniors all have a significantly higher level of perceptions than freshmen compared to freshmen, with significant explanatory power. \(R^{2}\)=0.032, \(F\)=12.054. science and engineering had higher values and total mental health for art and physical education students, \(t\)=3.205, \(P\)=0.045. liberal arts had higher values, behavioral performance, and total mental health for art and physical education students compared to art and physical education students, \(Beta\)=0.367, with significant positive predictive power.
Given that graduates are capable of providing a more objective and equitable assessment of the university’s student training and management practices, the statistical data and specific outcomes of the survey are presented in the following sections.
As depicted in Table 4, six indicators are presented: professional practice ability, social activity ability, organization and management ability, interpersonal communication ability, psychological quality, and behavioral performance ability. These indicators reflect the outcomes of the student management model. Notably, over 50% of graduates have demonstrated notable improvement in these six indicators during their academic tenure, with the index value for professional practice ability specifically reaching 76.1%. This underscores the efficacy of the current management model in fostering the holistic development of students.The student management model prioritizes psychological quality as its cornerstone, thereby broadening the scope of student management. It enhances the availability of elective courses and “second classroom” activities, reinforces mental health education, expands students’ understanding of mental health, fosters their adaptability, and comprehensively elevates their overall quality.
This paper advocates the integration of mental health education and student management through the employment of the SAFER-R model. To achieve this, we propose utilizing data mining technology to meticulously analyze students’ mental health status. Based on these insights, we suggest implementing personalized management strategies tailored to individual students’ mental health needs. Furthermore, we aim to establish a comprehensive, school-based mental health education and management framework, thereby facilitating the collaborative management of mental health education and student affairs under the umbrella of the collaborative education model. Ultimately, our endeavor seeks to innovate and enrich the collaborative education model.
Unifying the information of students’ mental health status and using Apriori algorithm to assess students’ mental health status, we get that students suffering from obsessive-compulsive disorder are very likely to have symptoms of depression, anxiety, interpersonal sensitivity and paranoia as well. The probability of students with symptoms of interpersonal sensitivity to somatization and paranoia is also higher. Combined with the visual presentation of students’ mental health data, the mental health status of students in this school is characterized by the prominence of obsessive-compulsive symptoms, followed by interpersonal sensitivity, depression and anxiety. Using gender, grade and major as independent variables, male students have more negative values and female students have healthier values compared to female students, \(R^{2}\)=0.023, \(F\)=5.351, \(Beta\)=-0.125, \(t\)=-3.826, \(P\)=0.043.
The collaborative parenting model-based mental health education and student management approach can enhance students’ comprehensive development capabilities across six key indicators: professional competency, social engagement skills, organizational and leadership abilities, interpersonal communication proficiency, psychological resilience, and behavioral conduct. This model fosters the holistic development of students.These six indicators were higher than 50 percent of the graduates.
In future research endeavors, we aim to explore methods for early identification of students’ mental health issues leveraging data analysis techniques, while simultaneously discussing potential preventive strategies. Moreover, we will acknowledge the inherent complexity and variability of the data and delve into the potential challenges associated with the application of data mining technologies in mental health education, notably privacy concerns and algorithmic biases. Furthermore, to enhance the comprehensiveness of our perspective, we propose to incorporate diverse viewpoints from a broader range of stakeholders.